Atrioventricular (AV) dissociation occurs when two completely independent pacemaker sites become active and compete with one another. In most cases, the sinus node provides one pacemaker, while an ectopic focus—usually ventricular—provides the other. Less commonly, two ectopic pacemakers may compete.
Although most dissociation involves pacemakers in different chambers (atria and ventricles), it is also possible—though rare—for both pacemaker foci to arise within the same chamber (e.g., sinus node vs. an atrial ectopic focus, or two independent junctional pacemakers).
The faster pacemaker will dominate, but the relative rates often allow impulses from both pacemakers to intermittently activate the ventricles.
In the accompanying article, AV dissociation occurs during a ventricular tachycardia (VT), which helps secure the diagnosis.
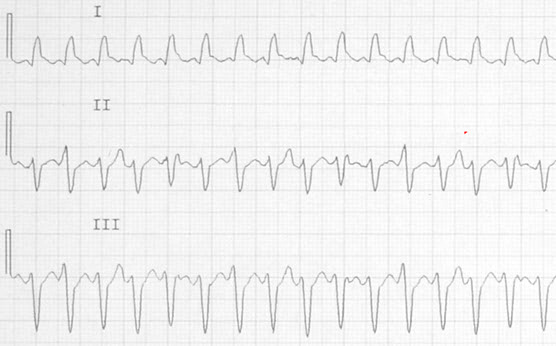
Most clinicians have only a vague idea of what they are looking for when scanning a wide complex tachycardia for signs of AV dissociation. This is not a simple task. It requires study, training, and a clear mental roadmap. AV dissociation will not be obvious, and it certainly will not jump out at you. You must look for it — and you must know exactly what you are looking for.
AV dissociation occurs when the atrial rhythm—usually sinus—continues to depolarize independently while a ventricular ectopic rhythm competes for control. Occasionally, a sinus impulse manages to conduct through the AV node and His bundle, reaching the ventricles when they are sufficiently repolarized. When this happens, the atrial impulse produces a conducted QRS complex: a capture beat.
You will see:
Capture beats are always early — never late.
Many online examples incorrectly label late beats as “capture beats.” Those are simply sinus beats occurring after the VT pauses. True capture beats interrupt the VT rhythm.
AV dissociation has a cousin: VA dissociation.
VA dissociation may or may not indicate VT.
AV dissociation, however, almost always indicates VT.
It is often taught as “absolute proof” of VT. It is not absolute — but the supraventricular rhythms capable of producing true AV dissociation are so rare that most clinicians will retire without ever seeing one. For practical purposes, AV dissociation is considered diagnostic of VT.
Look for a QRS that appears slightly too early.
A preceding P wave may or may not be visible; it is often buried in the T wave of the previous beat.
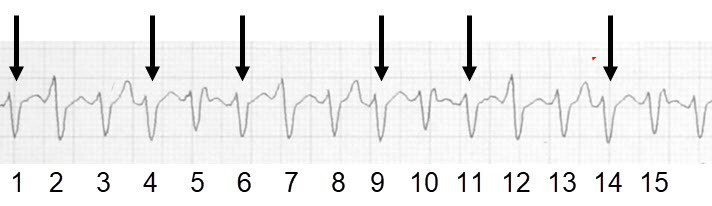
In the Lead II rhythm strip the arrowed QRS complexes represent the ventricular ectopic rhythm.
These are the exact places where sinus activity hides during AV dissociation.
Sinus P waves should be upright in all leads except aVR.
If a QRS appears early, it is likely a capture beat — even if the P wave is not visible.
During rapid rhythms, P waves are frequently swallowed by T waves. Always inspect the T wave of the preceding beat.
If you see a clear P wave followed by a QRS at a conductible PR interval — but the QRS appears late — that is not a capture beat. The VT simply paused long enough for normal conduction to occur. VT is notoriously paroxysmal.
Fusion beats are sinus‑conducted beats that activate the ventricles simultaneously with the ventricular ectopic focus. Because only part of the ventricles are captured, the resulting QRS is a hybrid.
Fusion beats:
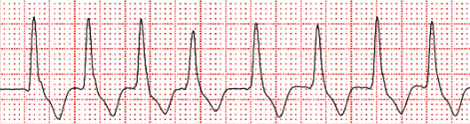
The fusion beat is the 4th beat — a small but real deviation from the surrounding VT morphology.