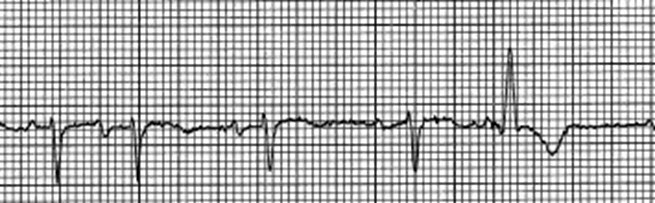
ECG Appearance
Typical features include:
- A wide QRS complex following a short R‑R interval that is preceded by a long R‑R interval
- RBBB‑type morphology (most common)
- Irregular coupling of aberrant beats
- Absence of a fully compensatory pause
- Occurrence during atrial fibrillation or other supraventricular rhythms with variable cycle lengths
These characteristics help differentiate Ashman aberrancy from ventricular ectopy.
Clinical Significance
Ashman–Gouaux Phenomenon is benign and represents normal physiology of the conduction system under varying cycle lengths. It does not require treatment, and management focuses on the underlying supraventricular rhythm, most commonly atrial fibrillation.
The primary clinical importance lies in recognition, as misinterpreting Ashman beats as ventricular arrhythmias may lead to unnecessary antiarrhythmic therapy, inappropriate cardioversion, or misdiagnosis of ventricular tachycardia.
A related concept, concealed perpetuated aberrancy (concealed transseptal conduction), explains why aberrant conduction may persist for several beats even after cycle lengths normalize, due to concealed retrograde penetration of the bundle branches.
Common Misinterpretations
Related Terms
- Rate‑dependent aberrancy
- Right bundle branch block
- Atrial fibrillation
- Concealed conduction
- Wide‑complex tachycardia (differential diagnosis)